Le cinque fasi del cambiamento
Il supporto comportamentale è parte importante di un tentativo per smettere di fumare e dovrebbe essere raccomandato a tutti i soggetti che intendono smettere.INTRODUZIONE
Se consideriamo che il 40% dei consumatori di nicotina fa un tentativo per smettere di fumare ogni anno, ma di questi solo il 4-6% riesce a stare senza fumare, in totale solo il 2% riesce a smettere.
Un terzo dei tentativi che hanno avuto successo ha richiesto una terapia medica o psicologica per raggiungere questo risultato.
I medici devono essere di supporto e capire i desideri dei pazienti, e capire che l’utilizzo del metodo delle 3A può offrire qualche beneficio. La comprensione delle Fasi del Cambiamento permette agli operatori sanitari di intervenire in modo mirato.
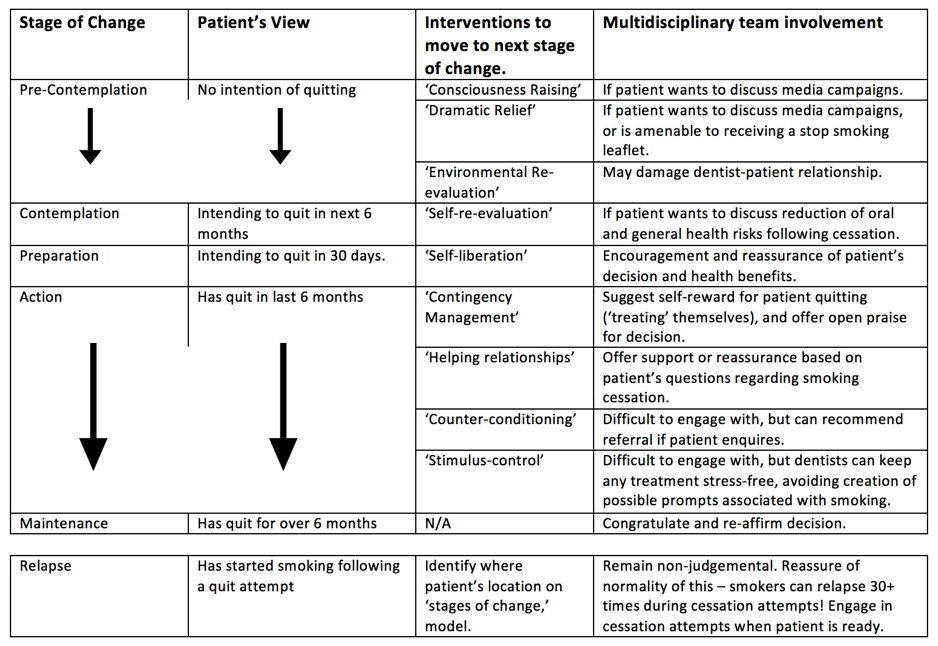
L’idea che il processo di astensione dal fumo poteva essere diviso in cinque fasi è stata descritta per la prima volta da Prochaska e DiClemente nel 1983, con possibili interventi per permettere progressi ai soggetti coinvolti attraverso le 5 fasi elencate nella tabella sottostante.
5 FASI DEL CAMBIAMENTO
PRE CONTEMPLAZIONE
In questa fase un individuo non ha intenzione di cambiare le sue abitudini a breve termine situazione che probabilmente rimarrà invariata per i prossimi mesi. Prevale un atteggiamento difensivo, evitando di pensare o parlare del loro comportamento ad alto rischio.
Non considerano il cambiamento perché sono demoralizzati dai precedenti tentativi di smettere, non capiscono le conseguenze delle loro azioni o credono che le conseguenze siano insignificanti. In poche parole, in questa fase i pro di fumare sono superiori ai contro. Per superare questo stadio bisogna riconoscere che le proprie azioni sono problematiche e potenzialmente dannose anche per chi sta attorno.
CONTEMPLAZIONE
In questa fase, l’individuo ha intenzione di cambiare il suo comportamento “a rischio” nei successivi sei 6 mesi. Cresce il sentimento di colpa per le proprie azioni e di quanto possano essere negative per la salute.
I soggetti in questa fase sono consapevoli del rischio delle loro azioni, ma non sono disposti a cambiare, sono in stato di incertezza pesando pro e contro.
PREAPARAZIONE
In questa fase, l’individuo ha pianificato di cambiare il suo comportamento dannoso in un mese. Questa fase del cambiamento di solito è composta da individui che hanno provato a smettere di fumare nei precedenti 12 mesi, ma hanno ricominciato e adesso si stanno impegnando a smettere di nuovo.
L’individuo deve decidere una strategia che miri a raggiungere il risultato desiderato. Come molti in questa fase ha provato a cambiare comportamento una volta (o più volte) in poassato, faranno ogni volta qualcosa di diverso per passare alla fase successiva, la fase dell’Azione.
AZIONE
In questa fase l’individuo ha cambiato il suo comportamento dannoso nei sei mesi precedenti. Riceverà i complimenti da parte di molte persone per gli sforzi fatti ma troverà anche questa fase la più difficile a causa dei sintomi di astinenza.
E’ necessario che si rimanga nella fase di azione fino a quando non è raggiunta una condizione di “auto-efficacia”, in questo modo si ha la forza per resistere alla tentazione di riprendere a fumare.
MANTENIMENTO
In questa fase l’individuo ha smesso di fumare da 6 mesi. La soddisfazione per aver smesso di fumare autoalimenta l’astensione dal fumo. Se la tentazione è troppo forte, o i pro a favore del fumo iniziano ad essere troppi, l’individuo abbandonerà la fase di mantenimento.
La maggior parte delle ricadute durante la fase di mantenimento avviene in presenza di altri fumatori, per questo si tende ad evitare la compagnia di gente che fuma. Chi non riprende a fumare rimane nella fase di mantenimento.
In soggetti con un passato di dipendenza è sempre possibile la ricaduta.

RECIDIVA
Pur non essendo una delle 5 fasi del cambiamento, è importante sottolineare come non tutti riescono a raggiungere la fase di mantenimento, e quelli che ce la fanno non è scontato che ci rimangano. Gli individui in queste condizioni hanno avuto delle ricadute e hanno ripreso a fumare. Ritorna a fumare di solito chi ha poca fiducia in se stesso o è poco convinto.
Per evitare le ricadute, è importante aiutare a ricordare perché si è deciso di smettere all’inizio. Le ricadute sono parte integrante del processo di cambiamento ed è importante rassicurare questi soggetti allo stesso modo degli altri.
Un individuo può riprendere a fumare più di 30 volte nel periodo in cui prova a smettere di fumare
COME INTERAGIRE CON UN FUMATORE
Bibliografia e letture di approfondimento
Bandura A. Self-efficacy mechanism in human agency. American psychologist. 1982 Feb;37(2):122.
Center for Disease Control and Prevention. Cigarette smoking among adults—United States, 1998. Morb Mortal Wkly Rep. 2000;49:881–4.
Chaiton M, Diemert L, Cohen JE, Bondy SJ, Selby P, Philipneri A, Schwartz R. Estimating the number of quit attempts it takes to quit smoking successfully in a longitudinal cohort of smokers. BMJ Open. 2016 Jun 1;6(6):e011045.
Cohen S, Lichtenstein E, Prochaska JO, et al. Debunking myths about self-quitting. Am Psychol. 1989;44:1355–65.
Cornuz J, Willi C. Nonpharmacological smoking cessation interventions in clinical practice. European respiratory review. 2008 Dec 1;17(110):187-91.
Ferguson SG, Frandsen M, Dunbar MS, Shiffman S. Gender and stimulus control of smoking behavior. Nicotine & Tobacco Research. 2015 Apr 1;17(4):431-7.
Fiore MC, Jaen CR, Baker TB, Bailey WC, Benowitz N, Curry SJ. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville MD: US Department of Health and Human Services, Public Health Service; 2008.
Foss R. Personality, social influence and cigarette smoking. J Health Soc Behav 1973; 14(3):279–286.
Higgins ST, Petry NM. Contingency management incentives for sobriety. Alcohol research & health. 1999 Mar 22;23(2):122-.
Hughes JR, Burns DM. Population Based Smoking Cessation. Bethesda, MD: National Cancer Institute;; 2001. Impact of medications on smoking cessation; pp. 155–64. Proceedings of a Conference on What Works to Influence Cessation in the General Population, Smoking and Tobacco Control, Monograph No. 12.
Hughes JR. Four beliefs that may impede progress in the treatment of smoking. Tobacco Control. 1999 Sep 1;8(3):323-6.
Humphreys K, Mankowski ES, Moos RH, Finney JW. Do enhanced friendship networks and active coping mediate the effect of self-help groups on substance abuse?. Annals of Behavioral Medicine. 1999 Mar 1;21(1):54-60.
Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. The Cochrane Library. 2005 Jan 1.
Lenio JA. Analysis of the Transtheoretical Model of behavior change. Journal of Student research. 2006;5:73-87.
Levesque DA, Cummins CO, Prochaska JM, Prochaska JO. Stage of Change for Making an Informed Decision about Medicare Health Plans. Health Services Research. 2006 Aug;41(4 Pt 1):1372.
Lindhe Söderlund, L. Motivational Interviewing in Theory and Practice. Digitala Vetenskapliga Arkivet 2010; 1198(): . http://www.diva-portal.org/smash/record.jsf?pid=diva2%3A356212&dswid=-6521 (accessed 10/11/16).
McNeill A., Raw M., Bauld L., Coleman T. (Guest Editors). Smoking treatment services in England: implementation and outcomes. Addiction 2005; 100
Moore M, Highstein G, Tschannen-Moran B, Silverio G. Coaching behavior change. Coaching: Psychology manual. 2010:33-51.
Morphett K, Partridge B, Gartner C, Carter A, Hall W. Why don’t smokers want help to quit? A qualitative study of smokers’ attitudes towards assisted vs. unassisted quitting. International journal of environmental research and public health. 2015 Jun 10;12(6):6591-607.
Orleans CT, Schoenbach VJ, Wagner EH, Quade D, Salmon MA, Pearson DC, Fiedler J, Porter CQ, Kaplan BH. Self-help quit smoking interventions: effects of self-help materials, social support instructions, and telephone counseling. Journal of consulting and clinical psychology. 1991 Jun;59(3):439.
Patten S, Vollman A, Thurston W. The utility of the transtheoretical model of behavior change for HIV risk reduction in injection drug users. Journal of the Association of Nurses in AIDS Care. 2000 Feb 29;11(1):57-66.
Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: applications to addictive behaviors. American psychologist. 1992 Sep;47(9):1102.
Prochaska JO, DiClemente CC. Stages and Processes of Self-Change of Smoking: Toward an Integrative Model of Change. Journal of Consulting and Clinical Psychology. 1983 Jun;51(3):390-95.
Prochaska JO, DiClemente CC. The transtheoretical approach. Handbook of psychotherapy integration. 2005 Feb 24;2:147-71.
PrOchaska JO, Prochaska JM. Behavior change. Population health: creating a culture of wellness. 2010 Oct 25.
Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. American journal of health promotion. 1997 Sep 1;12(1):38-48.
Prochaska JO. Transtheoretical model of behavior change. InEncyclopedia of behavioral medicine 2013 (pp. 1997-2000). Springer New York.
Raw M, McNeill A, Murray R. Case studies of tobacco dependence treatment in Brazil, England, India, South Africa and Uruguay. Addiction. 2010 Oct 1;105(10):1721-8.
Roddy E, Antoniak M, Britton J, Molyneux A, Lewis S. Barriers and motivators to gaining access to smoking cessation services amongst deprived smokers–a qualitative study. BMC Health Services Research. 2006 Nov 6;6(1):1.
Royal College of Physicians. Nicotine Addition in Britain. London, United Kingdom: Royal College of Physicians; 2000.
Siqueira LM, Rolnitzky LM, Rickert VI. Smoking cessation in adolescents: the role of nicotine dependence, stress, and coping methods. Archives of pediatrics & adolescent medicine. 2001 Apr 1;155(4):489-95.
Smith AL, Carter SM, Chapman S, Dunlop SM, Freeman B. Why do smokers try to quit without medication or counselling? A qualitative study with ex-smokers. BMJ open. 2015 Apr 1;5(4):e007301.
Stead LF, Lancaster T. Group behaviour therapy programmes for smoking cessation. Cochrane Database Syst Rev. 2005 Apr 18;2(2).
Taylor T, Lader D, Bryant A, Keyse L, Joloza MT. Smoking-related Behaviours And Attitudes 2005. London, United Kingdom: Office for National Statistics; 2005.
Tseng YH, Jaw SP, Lin TL, Ho CC. Exercise motivation and processes of change in community-dwelling older persons. Journal of Nursing Research. 2003 Dec 1;11(4):269-76.
U.S. Department of Health and Human Services (USDHHS). Reducing the health consequences of smoking: 25 years of progress. A report of the Surgeon General. Rockville (MD): U.S. Department of Health and Human Services, Centers for Disease Control, Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 1989. DHHS Pub. no. CDC 89-8411
Uppal N, Shahab L, Britton J, Ratschen E. The forgotten smoker: a qualitative study of attitudes towards smoking, quitting, and tobacco control policies among continuing smokers. BMC public health. 2013 May 3;13(1):1.
Velicer WF, Prochaska JO, Fava JL, Norman GJ, Redding CA. Smoking cessation and stress management: applications of the transtheoretical model. Homeostasis. 1998;38:216-33.
Venters MH, Solberg LI, Kottke TE, Brekke M, Pechacek TF, Grimm RH, Jr. Smoking patterns among social contacts of smokers, ex-smokers, and never smokers: the Doctors Helping Smokers Study. Prev Med 1987; 16(5):626–635.
Zimmerman GL, Olsen CG, Bosworth MF. A’stages of change’approach to helping patients change behavior. American family physician. 2000 Mar 1;61(5):1409.
Photos
Incense smoke (4) by losvizzero. Available at https://www.flickr.com/photos/folcobanfi/779572643/in/photolist-2bTvMD-7LpFkX-wxYDHW-apKcq5-4z9LEf-51mjSz-d34hh3-jpJPNp-4z9NVY-4z5xaM-PA1fhn-5ZUDyw-Ba5ox-4z9LTQ-itvTyk-dugc8b-nRxSnx-feQRqR-615wyM-bkCZoR-7CPT5c-4GsjjS-82Hb92-pzhfxD-4z5wrn-4Mrq6v-mw9vPZ-oWEA5t-4z9Kkf-2vVkpu-dxfnkW-pSg4d2-Sq7YAw-5LDsTX-8qfzJA-2bTwa4-eg3hB-4jbxjT-7QJ4xL-9DvemK-8KGdUq-7TKDf5-p6CrVD-6meTqN-agyBXN-oMWnEK-ijBdaF-CqJyt-dPiCM2-ThKCrH Licensed under CC BY-NC-ND 2.0
Change by Lee Jing Xi. Available at https://www.flickr.com/photos/jinx_1303/2973888147/in/photolist-5wMXkz-dhXVe4-dijMPN-4CruYx-qm3sT-7hi9oa-4BrZcd-4DZJzU-5UdnQF-cnz2vq-8eHE6w-JZXJ7-48uEZ-7zmw8k-4HRkPv-BmgGd-nyNtB-e2EaPE-5vRXVk-5G9zSv-5Au5JJ-5CHqbA-dyp4kq-8fmKCS-2qqWSF-6Niqwn-BmgGS-BmgFH-ovriCL-7eqWu-6BH6Kq-du8yPb-6puo57-99vLQv-7hkdvW-T5x8Th-8YENrX-6aKEQv-e8uDwc-dcZaG7-69cbLV-qxXmxV-oD5tjD-bwGbQX-bWXcoF-61hvET-9G8ERM-4oPJUQ-bygTHu-JvCYcH Licensed under CC BY-NC-ND 2.0
Glowing Ribbons of Smoke – FREE Texture by Barbara Courouble. Available at https://www.flickr.com/photos/plumnutz/7856722696/in/photolist-3D1XVu-7QJ4xL-fQb8im-9DvemK-8KGdUq-cYgKW9-7TKDf5-p6CrVD-6meTqN-agyBXN-a2tMaF-5d9M4H-oMWnEK-dMdj2Z-ijBdaF-CqJyt-dPiCM2-aHzyKT-ThKCrH-5Fx1Hg-iNpH9k-2bY121-5wpy8u-64qbTH-kGzfFv-4U48mS-5CDWAC-8MCUGP-daTqKi-kLwRMT-oYnMVT-9M2DUT-njZdQ9-oMtdSN-jAaURw-bpZvVo-6vGnpm-dYtAmP-kGzoTa-oqZAZY-k2FMY1-e7c6Wz-ehp9Et-aEAJPk-kLygsC-9NEtYQ-o1ipRg-drQeLR-c5XXRL-9EbwvZ Licensed under CC BY-NC 2.0
Match by Bastain. Available at https://www.flickr.com/photos/bneumann/2821962797/in/photolist-5inidZ-6ZRk6-DRLd5-tTLsQ-Guvnh-n3Cze-6ZRcF-kmCVBR-wrFWU-4LSs4f-Stv2w8-e4WdZm-hSiuww-wrFTb-8qEyUE-96bp33-8MA2Ho-wrFR7-Fesxw-7FiEgb-oTvg81-9LHYoU-3JAFqN-4FdfTi-5mW5WX-ojMwb3-4NMjAP-ekG8N6-avzjPr-aM9jN-ehdEyD-8yn3xT-8Y8KDk-5ZYN8o-7CYU4u-qkTDS-6CbyhG-9hkQN-6ZQrq-HdcJ81-onzHTC-jJPLs-5inqxi-52sDX8-8qDitT-8PdRik-pXUR2Y-9RjSa-GrAe2g-ox3QH Licensed under CC BY-SA 2.0
LO SAPEVI CHE
Fumare sigarette rollate a mano è dannoso quanto fumare quelle preconfezionate. Infatti, ci sono prove che dimostrano che le condizioni.