O modelo de mudança das cinco fases
O apoio comportamental é uma parte importante de qualquer tentativa de cessação do tabagismo e deve ser recomendado para todos os indivíduos que pretendem parar de fumar.Introdução
Se considerarmos que 40% dos utilizadores de nicotina realizam uma tentativa de cessação anualmente, mas apenas 4-6% conseguem manter a abstinência, apenas 2% dos utilizadores de nicotina atingem a cessação total por ano.
Um terço das tentativas de cessação bem-sucedidas exigem terapia médica ou psicológica para terem um resultado de bem-sucedido.
Os profissionais devem ser solidários e compreender os desejos do paciente, ao mesmo tempo devem perceber que a utilização da abordagem do “3A”, de um conselho de cessação breve, pode oferecer algum benefício. Compreender o modelo ‘Etapas da Mudança’, permite que os profissionais de saúde intervenham adequadamente.
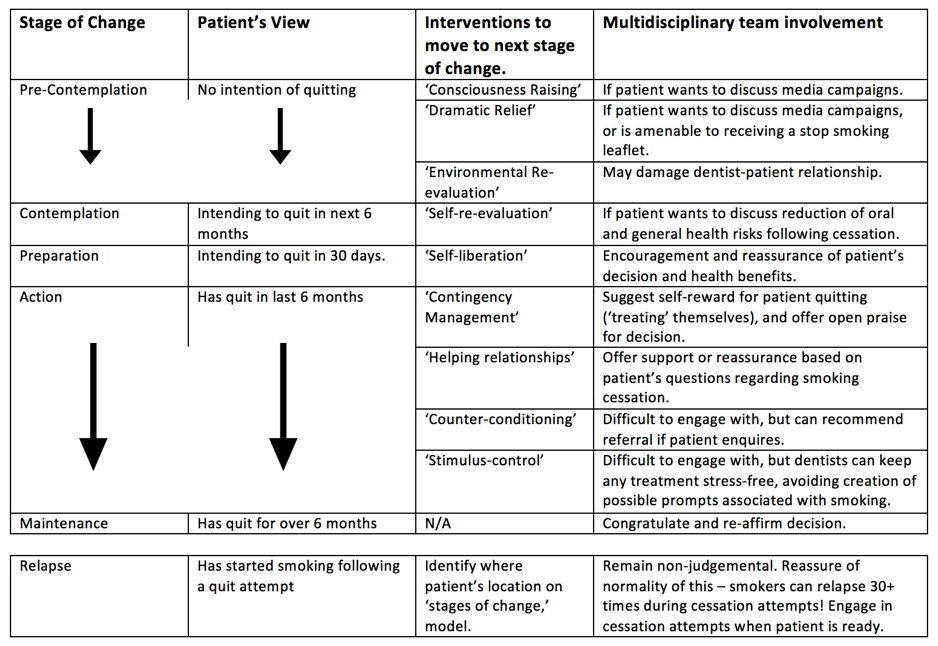
A sugestão de que a cessação tabágica poderia ser dividida em cinco etapas diferentes foi descrita pela Prochaska e DiClemente (1983), com potenciais intervenções para o progresso dos indivíduos nas 5 etapas descritas na tabela abaixo.
5 fases do modelo
Pré-Contemplação
Esta é a fase em que um indivíduo não tem intenção de alterar seu hábito no curto prazo (considerando-se os próximos seis meses). Nesta fase, os indivíduos geralmente são defensivos, evitando pensar ou falar sobre seu comportamento de alto risco.
Podem não estar a considerar a mudança pois estão desmoralizados com as tentativas de abandono anteriores, não entendem as consequências das suas ações ou acreditam que as consequências são insignificantes. Simplificando, nesta fase, e para o indivíduo os benefícios do tabagismo superam os malefícios de fumar. Para avançar a partir desta fase, o indivíduo deve aceitar que as suas ações são problemáticas e potencialmente prejudiciais para si e para os outros.
Contemplação
Nesta fase, o indivíduo pretende mudar o seu comportamento “de risco” nos próximos 6 meses. Os indivíduos ficam mais desiludidos com suas ações atuais e como elas podem prejudicar a sua saúde.
Nesta fase, o indivíduo estará ciente dos riscos inerentes às suas ações, mas, em última instância, não está disposto a mudar. O indivíduo está num estado de instabilidade, ponderando os prós e os contras.
Preparação
Nesta fase, o indivíduo planeia fazer a mudança longe do seu comportamento prejudicial no prazo de um mês. Geralmente consiste em indivíduos que tentaram mudar o seu comportamento “de risco” nos últimos 12 meses, mas recaíram e ainda estão envolvidos na atividade.
O indivíduo deve decidir/definir sobre qual a estratégia que resultará no resultado desejado. Como muitos, nesta fase, já tentaram mudar o seu comportamento uma vez (ou mais), geralmente adotarão um método diferente de progredir para a fase de ação.
Ação
Nesta fase, o indivíduo tomou a atitude de alterar o seu comportamento prejudicial nos últimos 6 meses. O indivíduo receberá os maiores elogios pelos seus esforços por parte dos outros, mas também achará esta fase a mais difícil devido aos sintomas de abstinência.
O indivíduo deve permanecer no estado de ação até que os sintomas transitem para um estado de “autoeficácia”, pois é mais forte do que a sua tentação de reverter o comportamento.
Manutenção
Esta fase de cessação do tabagismo pode ser simplesmente definida como aquela em que a pessoa não se envolveu no seu comportamento prejudicial por mais de 6 meses. A cessação contínua centra-se na satisfação do indivíduo na cessação. Se a tentação de fumar é muito grande, ou os pros do tabagismo começam a ser superados, o indivíduo recairá do estado de manutenção.
Mostra-se que a maioria das recidivas do estado de manutenção acontece na presença de outros fumadores e que indivíduos bem-sucedidos tendem a evitar situações sociais com outros fumadores. Aqueles que nunca fumam novamente permanecem no estágio de manutenção.

Recaída
Embora não seja uma das cinco fases do modelo de mudança, é importante notar que nem todos os indivíduos conseguem alcançar o estágio de manutenção, e aqueles que não conseguem lá permanecer. Todos os indivíduos em qualquer uma destas categorias diz ter “recaído”. Aqueles que recaem tendem a ser indivíduos que não têm grande convicção.
Para reverter a recaída, é importante que o indivíduo se lembre porque desistiu em primeiro lugar. As recaídas são uma parte normal do processo de mudança e aqueles que recaíram devem ser tranquilizados.
Um indivíduo pode ter até 30 recaídas durante a sua tentativa de parar de fumar.
How to interact with a smoker
Bibliografia e Leitura adicional
Bandura A. Self-efficacy mechanism in human agency. American psychologist. 1982 Feb;37(2):122.
Center for Disease Control and Prevention. Cigarette smoking among adults—United States, 1998. Morb Mortal Wkly Rep. 2000;49:881–4.
Chaiton M, Diemert L, Cohen JE, Bondy SJ, Selby P, Philipneri A, Schwartz R. Estimating the number of quit attempts it takes to quit smoking successfully in a longitudinal cohort of smokers. BMJ Open. 2016 Jun 1;6(6):e011045.
Cohen S, Lichtenstein E, Prochaska JO, et al. Debunking myths about self-quitting. Am Psychol. 1989;44:1355–65.
Cornuz J, Willi C. Nonpharmacological smoking cessation interventions in clinical practice. European respiratory review. 2008 Dec 1;17(110):187-91.
Ferguson SG, Frandsen M, Dunbar MS, Shiffman S. Gender and stimulus control of smoking behavior. Nicotine & Tobacco Research. 2015 Apr 1;17(4):431-7.
Fiore MC, Jaen CR, Baker TB, Bailey WC, Benowitz N, Curry SJ. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville MD: US Department of Health and Human Services, Public Health Service; 2008.
Foss R. Personality, social influence and cigarette smoking. J Health Soc Behav 1973; 14(3):279–286.
Higgins ST, Petry NM. Contingency management incentives for sobriety. Alcohol research & health. 1999 Mar 22;23(2):122-.
Hughes JR, Burns DM. Population Based Smoking Cessation. Bethesda, MD: National Cancer Institute;; 2001. Impact of medications on smoking cessation; pp. 155–64. Proceedings of a Conference on What Works to Influence Cessation in the General Population, Smoking and Tobacco Control, Monograph No. 12.
Hughes JR. Four beliefs that may impede progress in the treatment of smoking. Tobacco Control. 1999 Sep 1;8(3):323-6.
Humphreys K, Mankowski ES, Moos RH, Finney JW. Do enhanced friendship networks and active coping mediate the effect of self-help groups on substance abuse?. Annals of Behavioral Medicine. 1999 Mar 1;21(1):54-60.
Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. The Cochrane Library. 2005 Jan 1.
Lenio JA. Analysis of the Transtheoretical Model of behavior change. Journal of Student research. 2006;5:73-87.
Levesque DA, Cummins CO, Prochaska JM, Prochaska JO. Stage of Change for Making an Informed Decision about Medicare Health Plans. Health Services Research. 2006 Aug;41(4 Pt 1):1372.
Lindhe Söderlund, L. Motivational Interviewing in Theory and Practice. Digitala Vetenskapliga Arkivet 2010; 1198(): . http://www.diva-portal.org/smash/record.jsf?pid=diva2%3A356212&dswid=-6521 (accessed 10/11/16).
McNeill A., Raw M., Bauld L., Coleman T. (Guest Editors). Smoking treatment services in England: implementation and outcomes. Addiction 2005; 100
Moore M, Highstein G, Tschannen-Moran B, Silverio G. Coaching behavior change. Coaching: Psychology manual. 2010:33-51.
Morphett K, Partridge B, Gartner C, Carter A, Hall W. Why don’t smokers want help to quit? A qualitative study of smokers’ attitudes towards assisted vs. unassisted quitting. International journal of environmental research and public health. 2015 Jun 10;12(6):6591-607.
Orleans CT, Schoenbach VJ, Wagner EH, Quade D, Salmon MA, Pearson DC, Fiedler J, Porter CQ, Kaplan BH. Self-help quit smoking interventions: effects of self-help materials, social support instructions, and telephone counseling. Journal of consulting and clinical psychology. 1991 Jun;59(3):439.
Patten S, Vollman A, Thurston W. The utility of the transtheoretical model of behavior change for HIV risk reduction in injection drug users. Journal of the Association of Nurses in AIDS Care. 2000 Feb 29;11(1):57-66.
Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: applications to addictive behaviors. American psychologist. 1992 Sep;47(9):1102.
Prochaska JO, DiClemente CC. Stages and Processes of Self-Change of Smoking: Toward an Integrative Model of Change. Journal of Consulting and Clinical Psychology. 1983 Jun;51(3):390-95.
Prochaska JO, DiClemente CC. The transtheoretical approach. Handbook of psychotherapy integration. 2005 Feb 24;2:147-71.
PrOchaska JO, Prochaska JM. Behavior change. Population health: creating a culture of wellness. 2010 Oct 25.
Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. American journal of health promotion. 1997 Sep 1;12(1):38-48.
Prochaska JO. Transtheoretical model of behavior change. InEncyclopedia of behavioral medicine 2013 (pp. 1997-2000). Springer New York.
Raw M, McNeill A, Murray R. Case studies of tobacco dependence treatment in Brazil, England, India, South Africa and Uruguay. Addiction. 2010 Oct 1;105(10):1721-8.
Roddy E, Antoniak M, Britton J, Molyneux A, Lewis S. Barriers and motivators to gaining access to smoking cessation services amongst deprived smokers–a qualitative study. BMC Health Services Research. 2006 Nov 6;6(1):1.
Royal College of Physicians. Nicotine Addition in Britain. London, United Kingdom: Royal College of Physicians; 2000.
Siqueira LM, Rolnitzky LM, Rickert VI. Smoking cessation in adolescents: the role of nicotine dependence, stress, and coping methods. Archives of pediatrics & adolescent medicine. 2001 Apr 1;155(4):489-95.
Smith AL, Carter SM, Chapman S, Dunlop SM, Freeman B. Why do smokers try to quit without medication or counselling? A qualitative study with ex-smokers. BMJ open. 2015 Apr 1;5(4):e007301.
Stead LF, Lancaster T. Group behaviour therapy programmes for smoking cessation. Cochrane Database Syst Rev. 2005 Apr 18;2(2).
Taylor T, Lader D, Bryant A, Keyse L, Joloza MT. Smoking-related Behaviours And Attitudes 2005. London, United Kingdom: Office for National Statistics; 2005.
Tseng YH, Jaw SP, Lin TL, Ho CC. Exercise motivation and processes of change in community-dwelling older persons. Journal of Nursing Research. 2003 Dec 1;11(4):269-76.
U.S. Department of Health and Human Services (USDHHS). Reducing the health consequences of smoking: 25 years of progress. A report of the Surgeon General. Rockville (MD): U.S. Department of Health and Human Services, Centers for Disease Control, Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 1989. DHHS Pub. no. CDC 89-8411
Uppal N, Shahab L, Britton J, Ratschen E. The forgotten smoker: a qualitative study of attitudes towards smoking, quitting, and tobacco control policies among continuing smokers. BMC public health. 2013 May 3;13(1):1.
Velicer WF, Prochaska JO, Fava JL, Norman GJ, Redding CA. Smoking cessation and stress management: applications of the transtheoretical model. Homeostasis. 1998;38:216-33.
Venters MH, Solberg LI, Kottke TE, Brekke M, Pechacek TF, Grimm RH, Jr. Smoking patterns among social contacts of smokers, ex-smokers, and never smokers: the Doctors Helping Smokers Study. Prev Med 1987; 16(5):626–635.
Zimmerman GL, Olsen CG, Bosworth MF. A’stages of change’approach to helping patients change behavior. American family physician. 2000 Mar 1;61(5):1409.
Fotos
Incense smoke (4) by losvizzero. Available at https://www.flickr.com/photos/folcobanfi/779572643/in/photolist-2bTvMD-7LpFkX-wxYDHW-apKcq5-4z9LEf-51mjSz-d34hh3-jpJPNp-4z9NVY-4z5xaM-PA1fhn-5ZUDyw-Ba5ox-4z9LTQ-itvTyk-dugc8b-nRxSnx-feQRqR-615wyM-bkCZoR-7CPT5c-4GsjjS-82Hb92-pzhfxD-4z5wrn-4Mrq6v-mw9vPZ-oWEA5t-4z9Kkf-2vVkpu-dxfnkW-pSg4d2-Sq7YAw-5LDsTX-8qfzJA-2bTwa4-eg3hB-4jbxjT-7QJ4xL-9DvemK-8KGdUq-7TKDf5-p6CrVD-6meTqN-agyBXN-oMWnEK-ijBdaF-CqJyt-dPiCM2-ThKCrH Licensed under CC BY-NC-ND 2.0
Change by Lee Jing Xi. Available at https://www.flickr.com/photos/jinx_1303/2973888147/in/photolist-5wMXkz-dhXVe4-dijMPN-4CruYx-qm3sT-7hi9oa-4BrZcd-4DZJzU-5UdnQF-cnz2vq-8eHE6w-JZXJ7-48uEZ-7zmw8k-4HRkPv-BmgGd-nyNtB-e2EaPE-5vRXVk-5G9zSv-5Au5JJ-5CHqbA-dyp4kq-8fmKCS-2qqWSF-6Niqwn-BmgGS-BmgFH-ovriCL-7eqWu-6BH6Kq-du8yPb-6puo57-99vLQv-7hkdvW-T5x8Th-8YENrX-6aKEQv-e8uDwc-dcZaG7-69cbLV-qxXmxV-oD5tjD-bwGbQX-bWXcoF-61hvET-9G8ERM-4oPJUQ-bygTHu-JvCYcH Licensed under CC BY-NC-ND 2.0
Glowing Ribbons of Smoke – FREE Texture by Barbara Courouble. Available at https://www.flickr.com/photos/plumnutz/7856722696/in/photolist-3D1XVu-7QJ4xL-fQb8im-9DvemK-8KGdUq-cYgKW9-7TKDf5-p6CrVD-6meTqN-agyBXN-a2tMaF-5d9M4H-oMWnEK-dMdj2Z-ijBdaF-CqJyt-dPiCM2-aHzyKT-ThKCrH-5Fx1Hg-iNpH9k-2bY121-5wpy8u-64qbTH-kGzfFv-4U48mS-5CDWAC-8MCUGP-daTqKi-kLwRMT-oYnMVT-9M2DUT-njZdQ9-oMtdSN-jAaURw-bpZvVo-6vGnpm-dYtAmP-kGzoTa-oqZAZY-k2FMY1-e7c6Wz-ehp9Et-aEAJPk-kLygsC-9NEtYQ-o1ipRg-drQeLR-c5XXRL-9EbwvZ Licensed under CC BY-NC 2.0
Match by Bastain. Available at https://www.flickr.com/photos/bneumann/2821962797/in/photolist-5inidZ-6ZRk6-DRLd5-tTLsQ-Guvnh-n3Cze-6ZRcF-kmCVBR-wrFWU-4LSs4f-Stv2w8-e4WdZm-hSiuww-wrFTb-8qEyUE-96bp33-8MA2Ho-wrFR7-Fesxw-7FiEgb-oTvg81-9LHYoU-3JAFqN-4FdfTi-5mW5WX-ojMwb3-4NMjAP-ekG8N6-avzjPr-aM9jN-ehdEyD-8yn3xT-8Y8KDk-5ZYN8o-7CYU4u-qkTDS-6CbyhG-9hkQN-6ZQrq-HdcJ81-onzHTC-jJPLs-5inqxi-52sDX8-8qDitT-8PdRik-pXUR2Y-9RjSa-GrAe2g-ox3QH Licensed under CC BY-SA 2.0
Did you Know
Smoking hand rolled cigarettes is just as dangerous as pre-made cigarettes. Indeed, there is evidence to suggest poorer health outcomes in those who roll their own cigarettes.