Aids to cessation
In Europe, 29% of individuals identify as smokers. Some countries within Europe have alarmingly high rates of tobacco use; 40% of Greek adults smoke regularly.Introduction
Smoking and chewing tobacco are directly related to 650,000 mortalities each year in Europe, which is roughly 14% of all deaths.
People have different needs when they attempt full cessation, with some requiring intensive interpersonal support with pharmacotherapy and others able to quit successfully by ‘going cold turkey.’
Physical withdrawal symptoms can be titrated through nicotine replacement therapy (NRT).
There are other medications which can be used alongside NRT to help maintain cessation in motivated individuals.
Examples of these include Buproprion, Varenicline, Clonidine and Nortryptiline which must be prescribed by specialist stop smoking services or medical professionals in the UK.
For people who need face to face support to assist with cessation, there are Stop Smoking Services which can offer counselling.
Unaided, studies show that the rate of smokers who succeed in quitting is typically 2-4%.
For those who utilise ‘Stop Smoking,’ services alongside pharmacotherapy, these rates can increase to 15-20%.
Stop Smoking Services
Effective communication during smoking cessation is one of the most important facets in encouraging reduction of potential harmful behaviours.
Various modalities of communication can be utilised in the cessation pathway; didactic presentations, video demonstration, practice exercises and case studies in both individual and group sessions. Telephone based interventions have also been shown to be beneficial compared to a self-quitting approach, with other technologies being shown to have benefit as well.
Individual therapy
involves face-to-face appointments with a trained cessation therapist. Intervention can vary in intensity, however there is no evidence that a more intense intervention increases cessation success. Motivational interviewing is an integral part of this approach and is a patient-centred, designed to be modified to the patient’s approach to cessation. The individual approach tends to include sessions over several weeks, with increased number and longer sessions shown to be more effective.
Group therapy
Telephone and Technological Support
Nicotine Replacement Therapy
All forms of nicotine replacement therapy have been shown to be beneficial in long term smoking cessation, almost doubling success rates. NRT can take the form of gum, skin patches, inhalers, lozenges alongside nasal and oral sprays. It is a frequent component of smoking cessation strategies as it reduces the physiological effects of cessation, providing nicotine to reduce the effects of withdrawal.
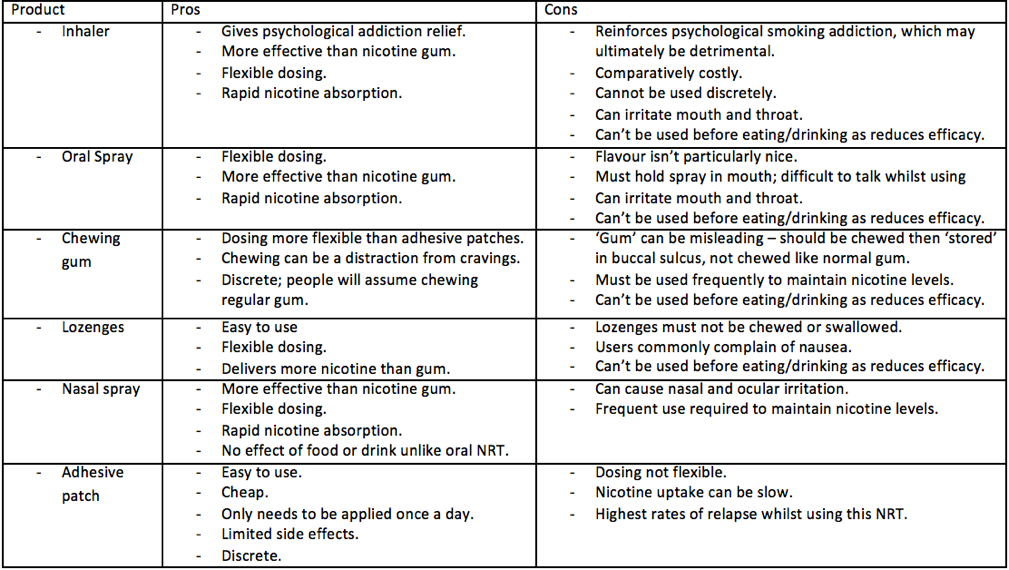
A Chart of Pros and Cons of different smoking cessation modalities
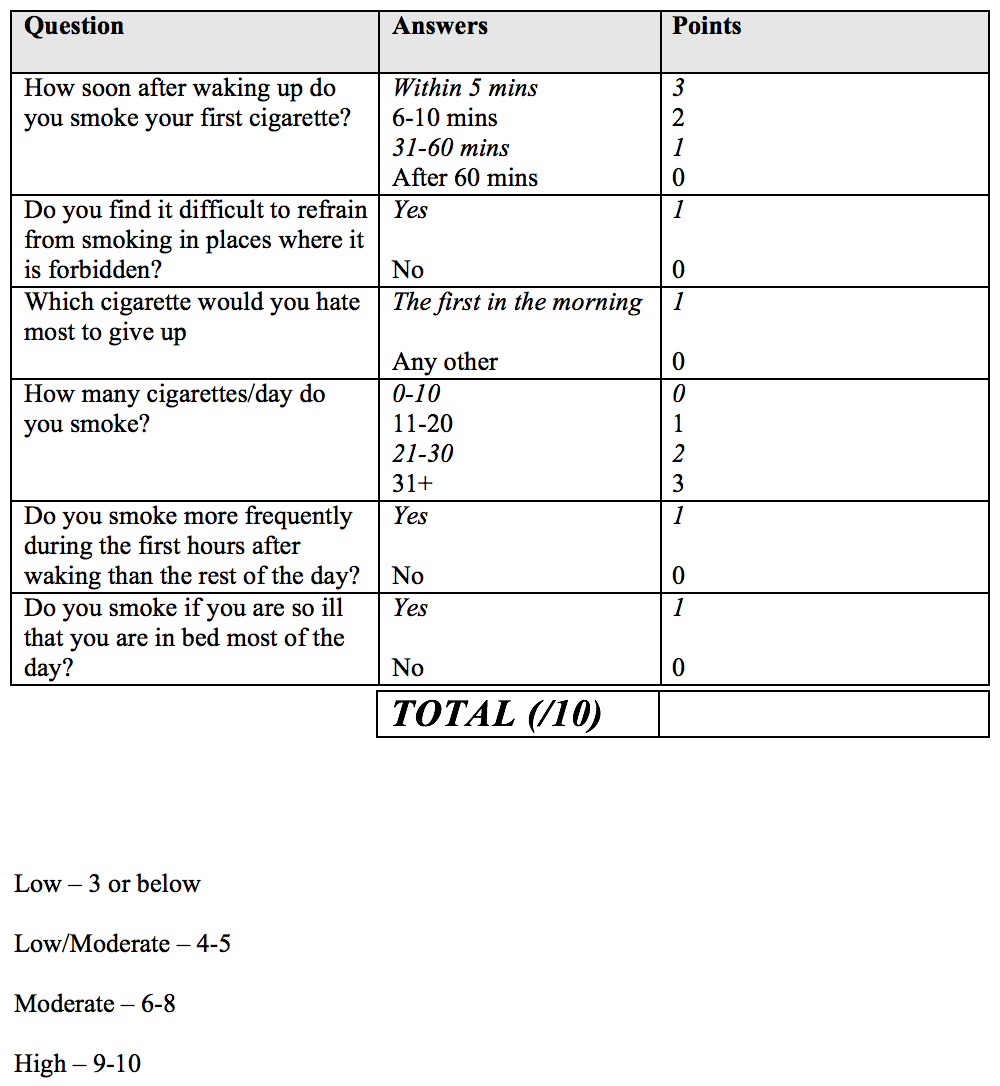
Heatherton’s adaptation of the Fagerstrom test of nicotine addiction.
Suggested NRT doseages, adapted from Government of Western Australia Department of Health Guidance

Pharmacotherapy (Varenicline, Buproprion, Clonidine & Nortriptyline)
Varenicline
Varenicline (Champix)
This drug blocks nicotinic receptors in the brain, removing the pleasurable sensations experienced upon having a cigarette. Any medicine which must be taken orally may result in side effects for the user.
Varenicline’s most common side effect is nausea, which is experienced by 33.5% of users.
There have been reports of more severe, neuropsychiatric adverse events such as depression and suicidal behaviour, however a literature search offers very limited evidence of such occurrences.
Buproprion
Buproprion (Wellbutrin)
Bupropion exerts its effect primarily through the inhibition of dopamine reuptake, which attenuates withdrawal symptoms by prolonging the presence of this neurotransmitter within neuronal synaptic vesicles.
The medication has been associated with manageable side effects such as nausea, dizziness and vomiting.
More serious side effects include hallucinations and seizures, although these are very rare, with the risk of seizures being reported by GlaxoSmithKline (2006) at 0.1%.
In relation to the two first line pharmacotherapy treatments, both have roughly the same amount of successful cessation after 2 years, although Varenicline seems slightly more effective in the short term.

Clondine and Nortriptyline
Second line pharmacotherapies; they iare given when the two first line therapies don’t work or are contraindicated.
These have both been shown to be roughly as effective as the first line medications, but have an increased number of side effects in most users.
In isolation, clonidine and nortryptiline have been shown to double quitting success.
Side effects are common in users and include:
- Clonidine: hypotension and drowsiness
- Nortriptyline: sedation, nausea, dry mouth, constipation, and urinary retention.
Did you Know
Each year, 3000 non-smokers die of lung cancer primarily caused by secondhand smoke. More than 33,000 non-smokers die of secondhand smoke-related heart disease.