The use of the 5 & 3 A's Protocol
The 5A’s approach to smoking cessation is the internationally accepted approach to brief intervention in nicotine users. The 3A's offers a condensed format for such intervention. Brief advice in primary care settings can increase succesful smoking cessation by 1-3%.Before we discuss the stages of the 5A’s and 3A’s, it is important to understand that different countries have different protocols to implement smoking cessation, and these are based on WHO Article 14 guidance in the Framework Convention on Tobacco Control.
WHO Guidelines
Article 14 (WHO 2003)
Demand reduction measures concerning tobacco dependence and cessation
- Each Party shall develop and disseminate appropriate, comprehensive and integrated guidelines based on scientific evidence and best practices, taking into account national circumstances and priorities, and shall take effective measures to promote cessation of tobacco use and adequate treatment for tobacco dependence.
- Towards this end, each Party shall endeavour to:
(a) design and implement effective programmes aimed at promoting the cessation of tobacco use, in such locations as educational institutions, health care facilities, workplaces and sporting environments;
(b) include diagnosis and treatment of tobacco dependence and counselling services on cessation of tobacco use in national health and education programmes, plans and strategies, with the participation of health workers, community workers and social workers as appropriate;
(c) establish in health care facilities and rehabilitation centres programmes for diagnosing, counselling, preventing and treating tobacco dependence; and
(d) collaborate with other Parties to facilitate accessibility and affordability for treatment of tobacco dependence including pharmaceutical products pursuant to Article 22. Such products and their constituents may include medicines, products used to administer medicines and diagnostics when appropriate.

These guidelines can be summarised by the ‘5 A’s’:
- Ask about and record smoking status.
- Advise smokers of the benefit of stopping in a personalised and appropriate way.
- Assess motivation to quit (using stages of change model).
- Assist smokers in their quit attempt.
- Arrange follow up with stop smoking services.
Advice from the healthcare practitioner does not have to be focussed on the minutiae of cessation and needs to only last three minutes.
Whilst knowledge of the treatment modalities to result in cessation are useful, ultimately the specialised stop smoking services will be able to adequately discuss any potential issues with the individual.
The 3 A’s Protocol
For practitioners who genuinely do not have time, a ‘3A’s’ approach may be acceptable. This can be summarised as follows:
- Ask and record smoking status.
- Advise patient of personal health benefits.
- Act on patient’s response.
This very brief advice can be delivered in less than one minute. There is an absence of conclusive evidence demonstrating the efficacy of 5A’s intervention over the 3A’s intervention, meaning either intervention is acceptable.
The healthcare environment can be very busy. The 3A’s approach is therefore a completely acceptable brief intervention.
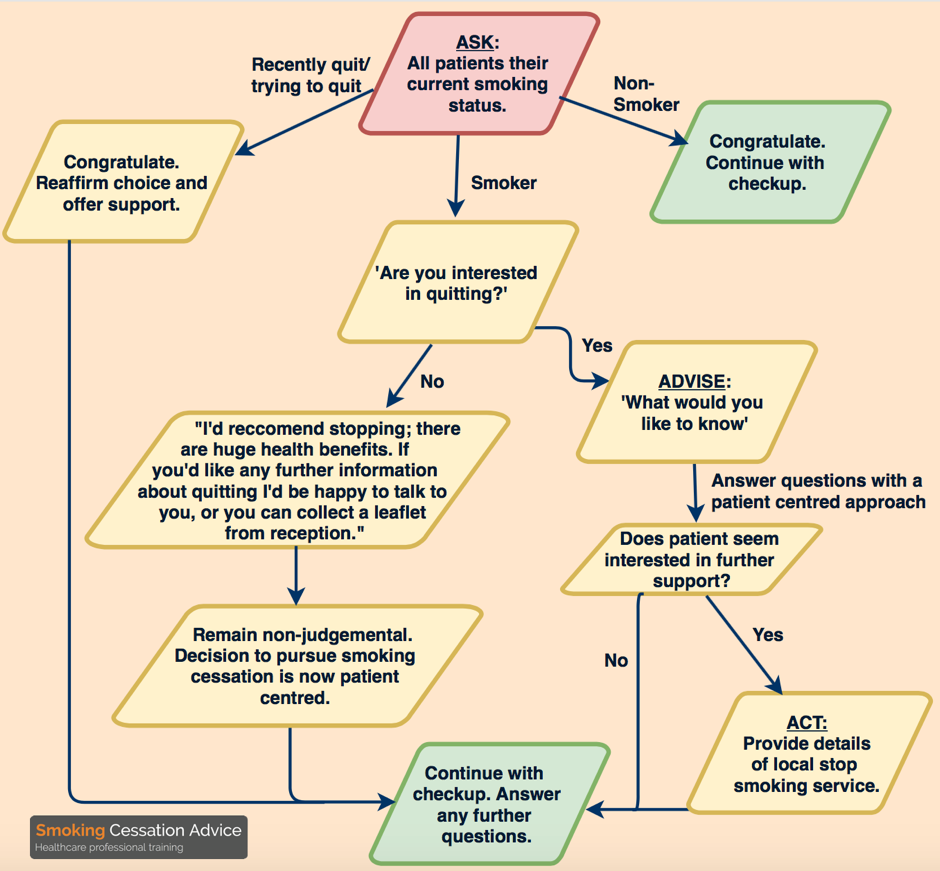
A flow chart outlining a conversation utilising the 3A's
Patient Centred Cessation
It is important to maintain the patient at the centre of any cessation attempt. We must therefore ensure that the practitioner focusses their approach on the responses of the patient.
For example, if the patient smokes, and does not wish to stop now, the healthcare professional must remain non-judgemental.
This allows the patient to plan their actions. If the patient is positive in their response, we recommend that the 3 A’s approach can be continued.
It is easier to implement the 3A’s in the fast-paced healthcare environment. It is shown that a healthcare professional’s approach to smoking cessation is central to its success.
Healthcare professionals should therefore act appropriately when discussing quitting with an addicted individual. Ultimately, the decision to contact stop smoking services can be made by the individual. Self-referral has been shown to be linked to increased success in cessation.
Bibliography and Further Reading
AL-Doghether MH. The Behavioural Interventions for Smoking Cessation. Asia Pacific Family Medicine. 2004 Jan 1;3(1-2):19-28.
Aveyard P. Keeping Smoking-Cessation Interventions Brief and Effective. Smoking Cessation Rounds. 2009;3(2).
Dawson GM, Noller JM, Skinner JC. Models of smoking cessation brief interventions in oral health. New South Wales public health bulletin. 2014 Jan 22;24(3):131-4.
Geneva, WHO. 2003. Framework convention on tobacco control. Available at: http://www.who.int/tobacco/framework/WHO_FCTC_english.pdf, accessed on Feb 14 2017
Gordon JS, Andrews JA, Crews KM, Payne TJ, Severson HH. The 5A’s vs 3A’s plus proactive quitline referral in private practice dental offices: preliminary results. Tobacco control. 2007 Aug 1;16(4):285-8.
McLeod D, Cornford E, Pullon S, de Silva K, Simpson C. Can Quit Practice: a comprehensive smoking cessation programme for the general practice team. The New Zealand Medical Journal (Online). 2005 Apr 15;118(1213).
Solberg LI, Kottke TE, Majeskie MR, Fiore MC, Baker TB. Patient perceptions: an important contributor to how physicians approach tobacco cessation. Tobacco control. 1998 Dec 1;7(4):421-3.
Photos
Question by Noelia. Available at https://www.flickr.com/photos/noeliabadillo/5545228214/in/photolist-9s1Ka1-afsoif-afpA84-asZokq-nX5GD-7bMUh3-jCR8bu-9XLKwe-5sWuny-7D1qMf-aoXtV-83Ako-cEWAkA-LmY5o-5G3KM-7CdjQ1-acVh1Z-4NCSef-9kX1eV-ahcPcQ-ukStnt-5DAUqj-24VHAL-8YaFEb-4nSWjf-apvTVA-9ksuae-RjyhqG-7yxzv4-eWrbm-9kstWR-7JK81m-afaffH-4NyCNc-dtxozY-5U8U2u-dtxokY-5ejEfU-CQ9xq-eEStnj-HpsZZ-egLaMo-bnCSSc-pQ19Vh-4d5HvK-XLaRW-c6o6vL-7KGEEp-7ME8ae-2UuhRG Licensed under CC BY-NC-ND 2.0
Quit by Joao Brizzi. Available at https://www.flickr.com/photos/joaobrizzi/8748825937/in/photolist-ek729v-dzs8vh-dznTDp-dzoRR8-dznQUn-dzuH4Q-dzthTw-dzowwx-dzurzG-dzni8V-dzuAgJ-dzsN6j-dztees-dzu1Z9-dzo82n-9YZRSq-dzpcLH-dzsJ43-dznZiR-dznS2M-dzth9u-dzo5EP-dznhsr-dB9wM1-dznRQg-dzumDh-dzuAsf-dzthsL-dzunQu-dzuPWj-dRrV9G-5vPicQ-7FQYV2-7qKFNn-7LaDqL-TyyPgR-5R7K6w-4ozN3D-dztfF3-dzundd-dzut97-dzowre-dzp4sr-dznRqv-dzp2up-dzp64X-dzteMG-dzttF7-dznTVc-dzs9Lf Licensed under CC BY-SA 2.0
Did you Know
Users of smokeless tobacco are exposed to higher amounts of tobacco-specific nitrosamines — molecules that are known to be carcinogenic — than smokers.